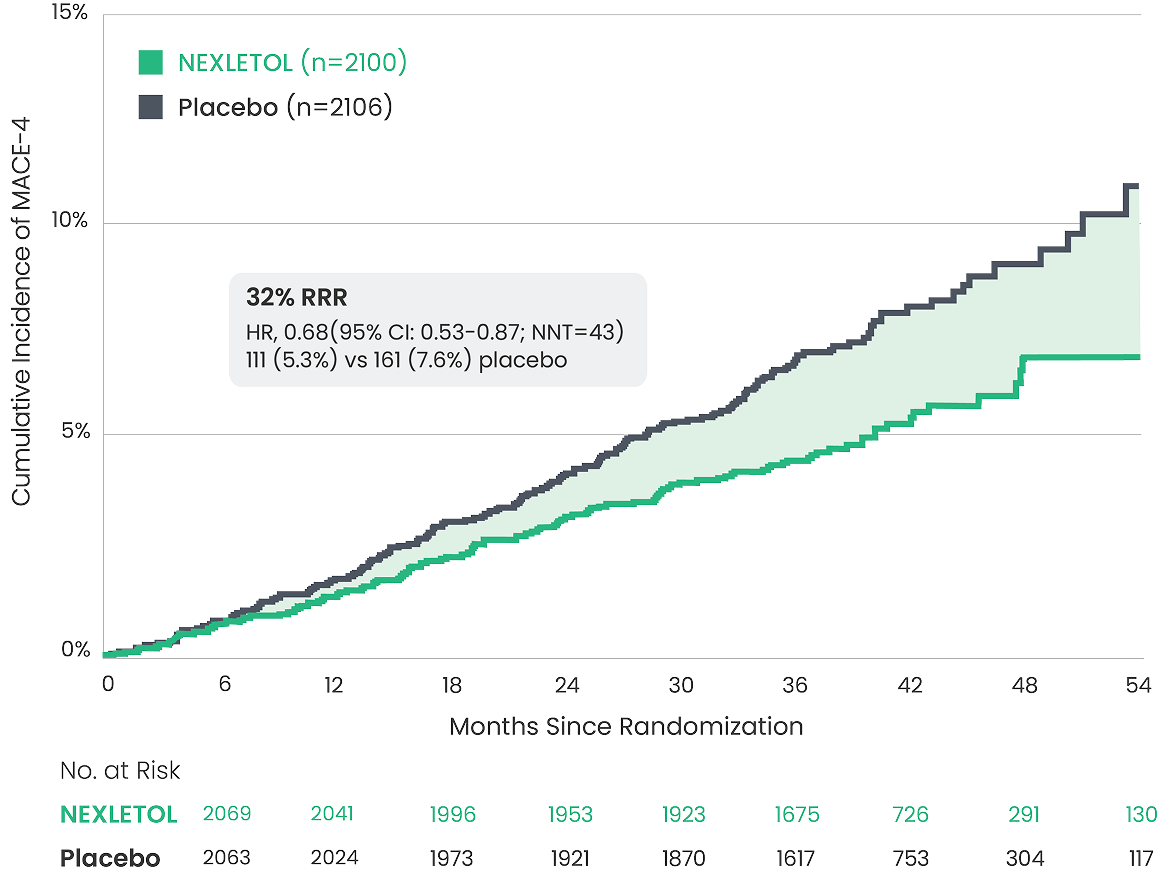
Primary Prevention Subgroup
Prespecified exploratory analysis of primary prevention patients1
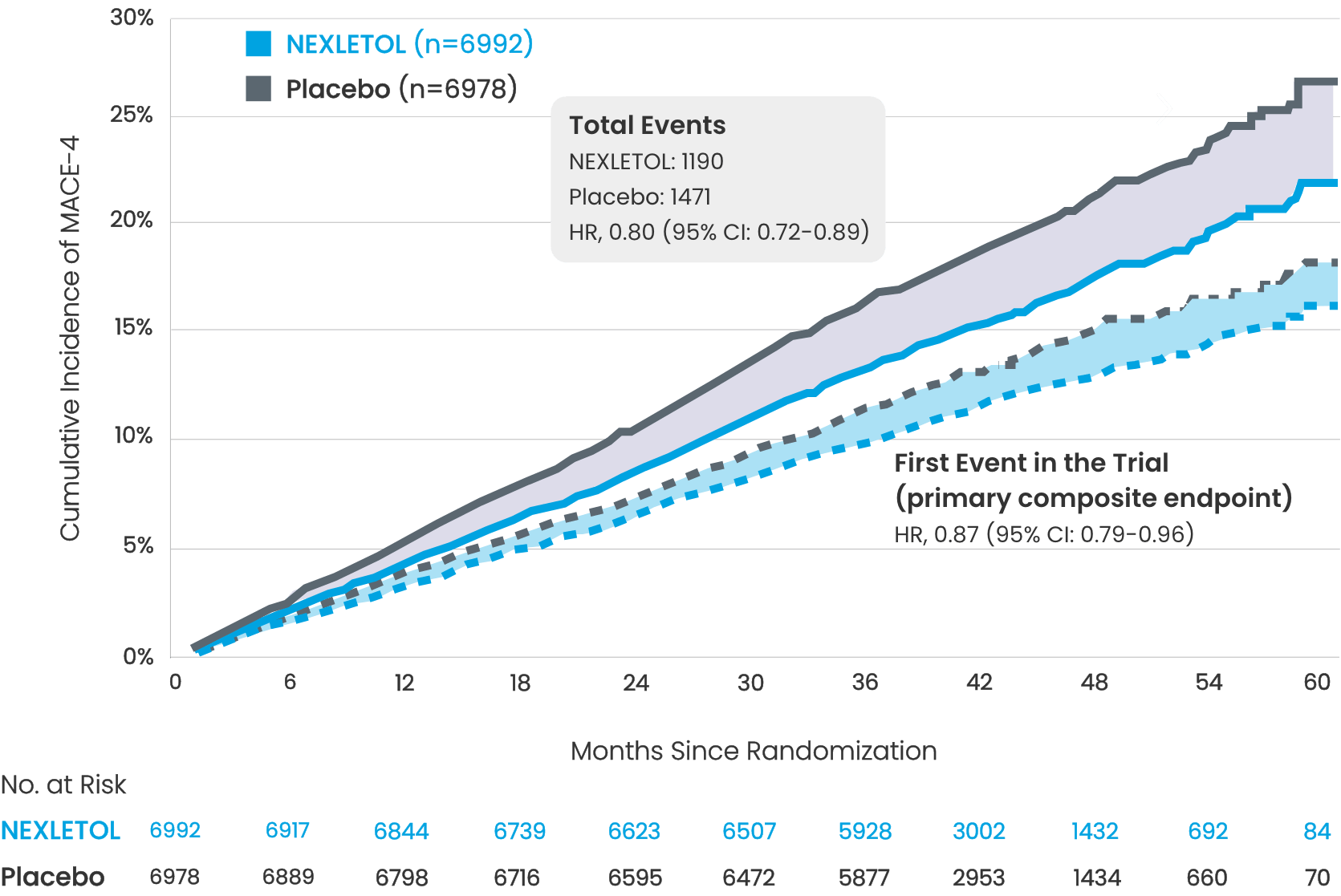
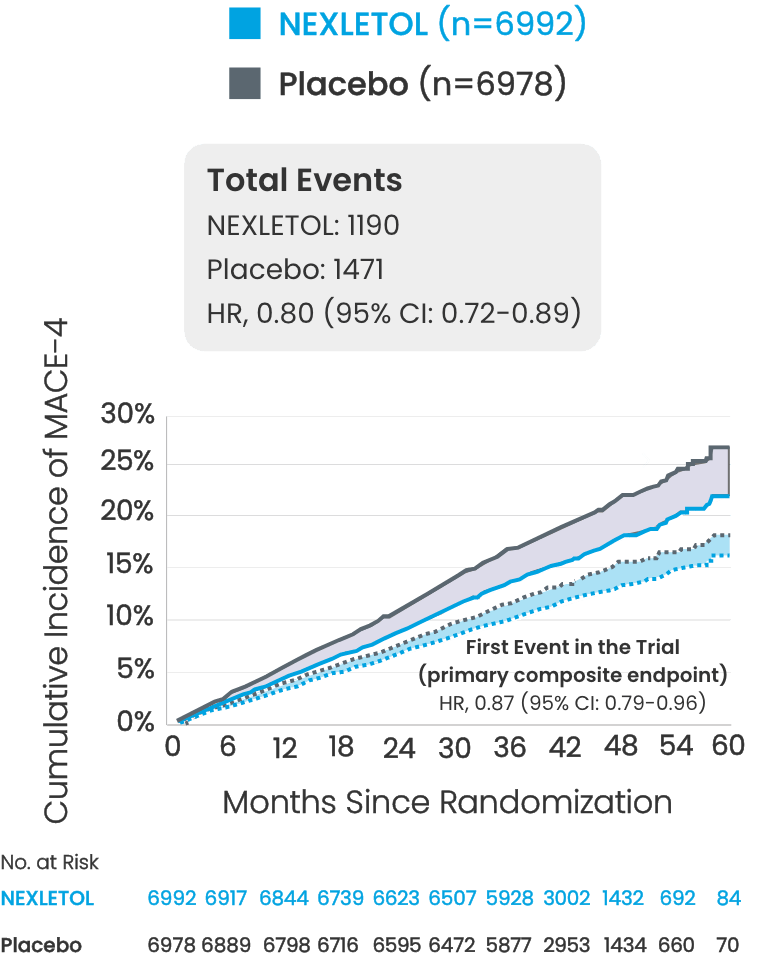
Time to First Occurrence of MACE-4 in Primary Prevention Patients2,3
(nonfatal MI, coronary revascularization, nonfatal stroke, or CV death)

MACE-34
(nonfatal MI, nonfatal
stroke, or CV death)
39
%
RRR
RRR
HR, 0.61
(95% CI: 0.46-0.80;
83 vs 134 placebo)
Nonfatal MI5
HR, 0.63
(95% CI: 0.39-1.01;
28 vs 44 placebo)
Coronary
Revascularization4
HR, 0.73
(95% CI: 0.50-1.05;
50 vs 68 placebo)